Abbott PV Present status and future directions: managing endodontic emergencies. Int Endod J. 2022; 55 Suppl 3:778-803 https://doi.org/10.1111/iej.13678
Cai C, Chen X, Li Y, Jiang Q Advances in the role of sodium hypochlorite irrigant in chemical preparation of root canal treatment. Biomed Res Int. 2023; 2023 https://doi.org/10.1155/2023/8858283
Shetty SR, Al-Bayati SAAF, Narayanan A Sodium hypochlorite accidents in dentistry. A systematic review of published case reports. Stomatologija. 2020; 22:17-22
Spencer HR, Ike V, Brennan PA Review: the use of sodium hypochlorite in endodontics–potential complications and their management. Br Dent J. 2007; 202:555-559 https://doi.org/10.1038/bdj.2007.374
Kleier DJ, Averbach RE, Mehdipour O The sodium hypochlorite accident: experience of diplomates of the American Board of Endodontics. J Endod. 2008; 34:1346-1350 https://doi.org/10.1016/j.joen.2008.07.021
Becking AG Complications in the use of sodium hypochlorite during endodontic treatment. Report of three cases. Oral Surg Oral Med Oral Pathol. 1991; 71:346-348 https://doi.org/10.1016/0030-4220(91)90313-2
Motta MV, Chaves-Mendonca MA, Stirton CG, Cardozo HF Accidental injection with sodium hypochlorite: report of a case. Int Endod J. 2009; 42:175-182 https://doi.org/10.1111/j.1365-2591.2008.01493.x
Witton R, Brennan PA Severe tissue damage and neurological deficit following extravasation of sodium hypochlorite solution during routine endodontic treatment. Br Dent J. 2005; 198:749-750 https://doi.org/10.1038/sj.bdj.4812414
Vianna ME, Gomes BP, Berber VB In vitro evaluation of the antimicrobial activity of chlorhexidine and sodium hypochlorite. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004; 97:79-84 https://doi.org/10.1016/s1079-2104(03)00360-3
Jeansonne MJ, White RR A comparison of 2.0% chlorhexidine gluconate and 5.25% sodium hypochlorite as antimicrobial endodontic irrigants. J Endod. 1994; 20:276-278 https://doi.org/10.1016/s0099-2399(06)80815-0
Emergency multidisciplinary management of a sodium hypochlorite injury in an adolescent: Case Report Mira Shah M Lawrence Kathleen Fan Dental Update 2025 52:1, 50-53.
Authors
MiraShah
BEng (Hons), BDS, MFDS RCS (Ed)
BEng (Hons), BDS, MFDS RCS (Ed), Specialist Trainee in Periodontology, King's College London
This case report describes the multidisciplinary team (MDT) management of a severe sodium hypochlorite (NaOCl) injury in a 16-year-old male caused by NaOCl extrusion during emergency extirpation of the UL2 without the use of a dental dam. Ophthalmology, oral and maxillofacial surgery (OMFS) and acute dental input were required to manage this patient during their 72-hour inpatient hospital admission. Plain film and CT imaging were used to assess the degree of NaOCl infiltration and guide treatment. Serial dilution using sterile saline irrigation intra-orally and extra-orally of the left eye was required to reduce the cytotoxicity of NaOCl.
CPD/Clinical Relevance: Clinicians should be aware of the potentially hazardous complications of NaOCl incidents, their clinical presentation and the importance of early recognition and management by an appropriate MDT.
Article
The COVID-19 pandemic heavily disrupted access to routine dental examinations and treatment. This resulted in a backlog in NHS routine dental services, increasing the prevalence of untreated dental diseases in the UK population. Dental caries, if untreated, can infiltrate deep into the pulp of a tooth resulting in acute pain and pulpal infection/inflammation. Such cases may require emergency extirpation treatment,1 commonly with the use of sodium hypochlorite (NaOCl) as the endodontic irrigant. This case report describes the multidisciplinary team (MDT) management of an NaOCl injury, a complication of extirpation treatment.
Case presentation
A 16-year-old male, otherwise fit and well with an allergy to penicillin, was referred to the oral and maxillofacial surgical (OMFS) on-call team by the emergency department of a different hospital 36 hours following extirpation of his upper left second incisor (UL2). The cause of the pre-existing lesion of the UL2 is unknown, but is likely to have been due to dental trauma. The patient attended hospital in pain with significant left-sided facial swelling, extra-oral ecchymosis, peri-orbital oedema and intra-oral ulceration. Prior to treatment the patient had been experiencing significant pain from the causative tooth for several months. Extirpation was performed by an emergency private dentist, using sodium hypochlorite as an irrigant, without the use of dental dam. Immediately following the procedure, the patient reported pain and intra-oral ulceration, with progressive facial swelling occurring the following morning. The patient had contacted the dental practitioner, but was unable to be reviewed by a dentist for a further week, owing to a lack of available appointments.
Clinical examination
On examination the patient was able to maintain his own airway with a respiratory rate of 15/minute and oxygen saturation of 99% on room air. Extra-orally, he had fluctuant left-sided facial and labial bruising and swelling that was erythematous and tender on palpation (Figure 1). Left peri-orbital swelling was associated with significant epiphora and subjective burning sensation of the left eye. He had no visual disturbances and free range of eye movements. Intra-orally there was ulceration affecting the upper left labial and gingival mucosa. He was otherwise apyrexial with a blood pressure of 132/75.
Figure 1. Initial presentation of the patient to OMFS taken in the emergency department after 300 mg IV clindamycin and 6.6 mg IV dexamethasone administered at a different emergency department.
Investigations and results
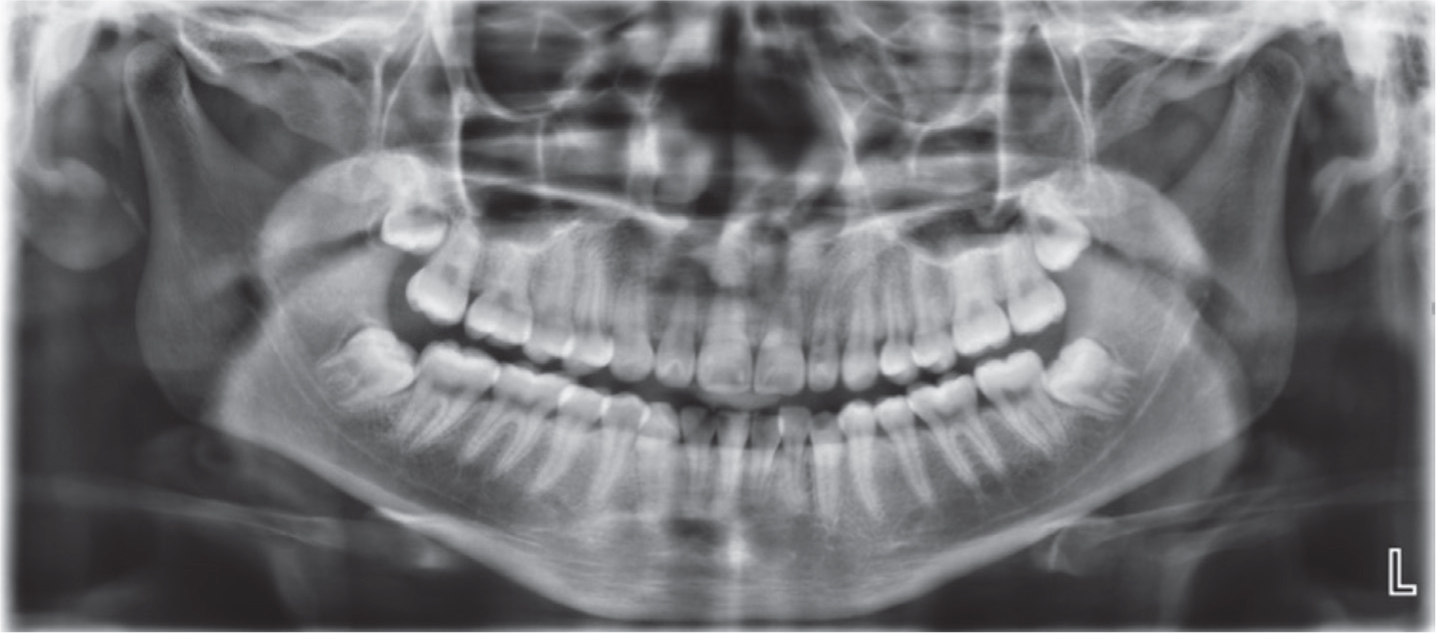
An orthopantomogram (OPG) (Figure 2) was taken as a baseline to assess the dentition involved and for any obvious apical pathology.
Figure 2. Orthopantomogram showing distal radiolucency of the UL2 suggestive of perforation.
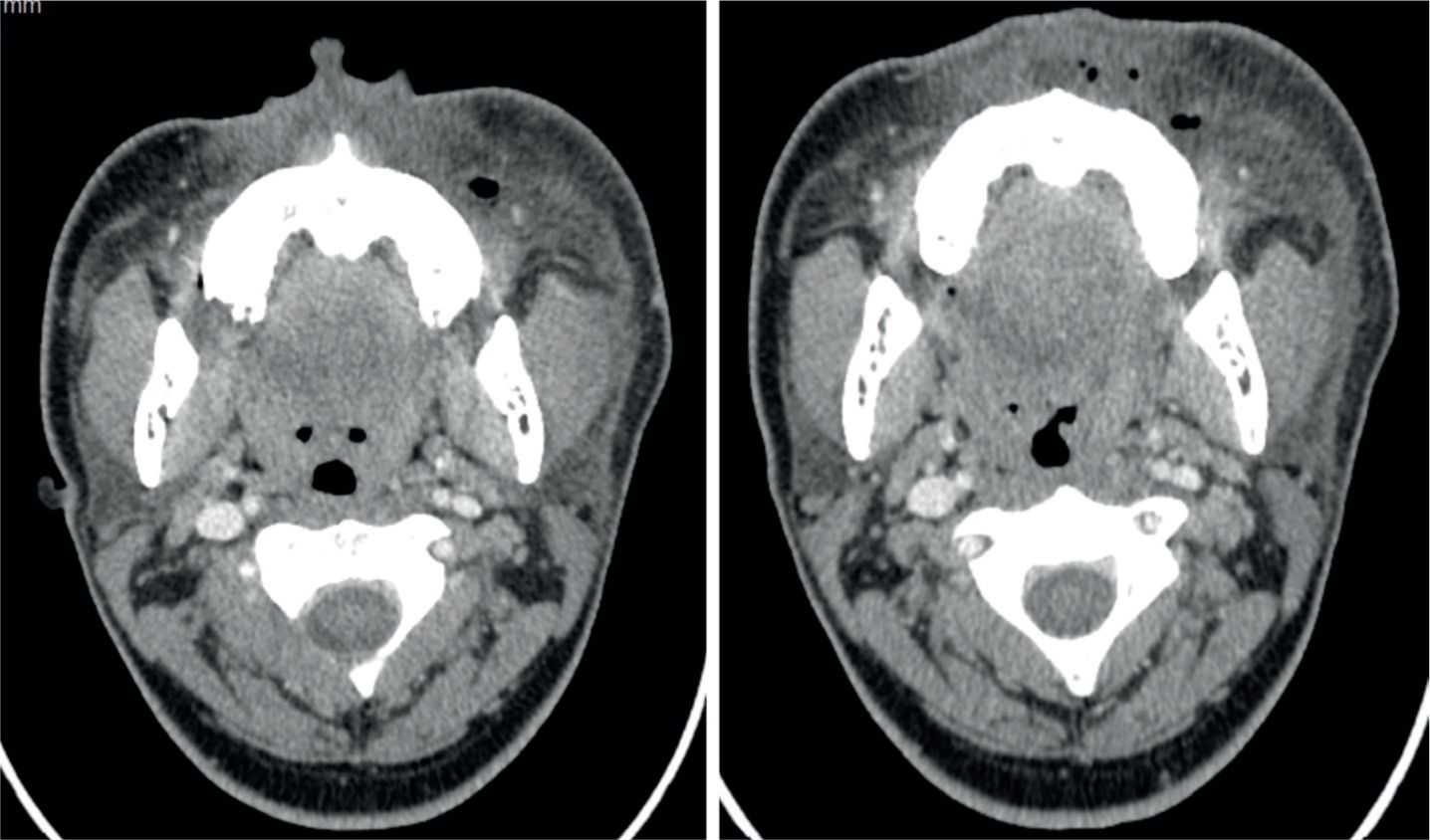
A CT of his facial bones and neck was used to further assess the extent of injury and to assess for any bony infiltration, soft tissue collections, haematomas or presence of surgical emphysema (air) (Figure 3). CT demonstrated a linear radiolucency within the UL2, with extensive subcutaneous oedema and inflammatory fat stranding involving the soft tissues just inferior to the left maxilla and extending to the superior alveolar ridge with multiple locules of gas within the subcutaneous tissues. There was no associated organized collection or changes in the appearance of the underlying bone.
Figure 3. Axial CT facial bone views showing extensive subcutaneous oedema and multiple locules of gas inferior to the left maxilla.
Management
Following clinical assessment and investigations, the patient was admitted under the care of the OMFS team for 3 days for coordinated management of his NaOCl-related facial injuries by the MDT. The patient was treated with 300 mg intravenous (IV) clindamycin every 6 hours, alongside IV paracetamol and two doses of 8-mg IV dexamethasone. Facial cooling therapy using the Hilotherm system (Hilotherm GmbH, Switzerland) was used for controlled, continuous cooling of the facial soft tissues to help reduce swelling by vasoconstriction, and provide pain relief. The left eye was initially flushed with 500 ml of sterile saline and monitored for signs of improvement.
Occular symptoms were managed by the ophthalmology team who prescribed topical 0.2% carbomer gel to the left eye as needed. After the patient declined dilation of the eye, in the context of clinical improvement, he was discharged from their care.
The temporary restoration of the UL2 was removed by the acute dental care department, and the canal flushed with copious amounts of sterile saline to dilute the NaOCl and neutralize the alkalinity of the NaOCl, preventing further cytotoxicity of tissues. Following treatment, the patient reported significant improvement and was discharged home with analgesia and 300 mg oral clindamycin to be taken four times daily for a further 7 days (Figure 4). Subsequent review of the patient 1 week later in the outpatient department demonstrated evidence of continued clinical resolution and improvement, allowing discharge of the patient back to the community.
Figure 4. Clinical photographs taken prior to discharge, showing significant reduction in left-side midfacial and labial swelling.
Discussion
During extirpation, endodontic irrigants are used as antimicrobial agents and to dissolve pulpal tissue. Sodium hypochlorite (NaOCl) is considered the gold standard and most widely used irrigant owing to its antimicrobial and saponification properties, and its ability to dissolve both vital and necrotic pulpal tissue.2 However, if it extrudes beyond the root canal system into the peri-radicular tissues, its cytotoxic activity can lead to ‘rapid haemolysis and ulceration, inhibition of neutrophil migration and destruction of endothelial and fibroblast cells’.3 This is known as an a NaOCl incident. The severity of the incident depends on the duration of exposure and concentration of NaOCl used. However, even a small amount of extrusion of NaOCl can result in peri-radicular inflammation. Shetty et al reported that the majority of NaOCl incidents occurred when 3% NaOCl was used.4 Further research is required to investigate whether a safe concentration of NaOCl exists.
Risk factors that increase the probability of sodium hypochlorite incidents include:
The use of a taper seat needle that may dislodge in use;
Incorrect positioning of the needle when it engages into the canal;
Protrusion of the needle further than the estimated working length of the prepared canal and a high-pressure delivery of the irrigant;
Lack of PPE for both patient and operator;
Incorrect use or absence of dental dam.5 It is therefore imperative that a dental dam is used to prevent contact between NaOCl and surrounding tissues.
Kleier et al reported a higher incidence of NaOCl injury in the maxilla compared to the mandible (P<0.0001) and affecting more posterior teeth than anterior ones (P>0.0001)6 owing to the low cortical bone thickness and high trabecular bone tissue. Additionally, females were more likely to experience NaOCl incidents than males.6 It has been hypothesized that this may be due to the increased bone density in the male population; however, there is a lack of high-quality scientific evidence to support this gender predilection.
Multiple authors5,7,8 have suggested the use of prophylactic antibiotic therapy to prevent the proliferation of bacteria in the peri-apical space containing necrotic tissue leading to secondary infection. However, Motta et al reported that antibiotics should only be administered if there is clinical evidence of wound infection or exposure.9 Simple analgesia such as 1000 mg paracetamol four times daily is recommended to manage mild to moderate pain.10 Aspirin and non-steroidal analgesia should not be used as first stage pain management owing to the presence of interstitial haemorrhage in the soft tissue.11 Steroid therapy can be used in severe injuries, such as the case described, to control the inflammatory reaction;8,12,13 however, the effectiveness of this is yet to be established. The use of a cold compress for the initial 24-hour period is advised to reduce oedema, inflammation and pain followed by warm compression for the next 24 hours.12Table 1 outlines recommendations on how to manage a NaOCl extrusion incident in a dental practice. It imperative that the patient is reassured and the incident documented in a comprehensive manner.
Immediate irrigation of the root canal using saline
Use of a cold compress for initial 24 hours
Use of a warm compress after the initial 24 hours
1000 mg paracetomal four times daily for management of mild to moderate pain
Monitor patient daily
The majority of patients are expected to make a full recovery; however, the time period of this grossly depends on the extent of injury and the time taken for presentation and commencement of management.
There is a lack of evidence to suggest that endodontic treatment cannot be completed following a NaOCl incident. However, it is highly recommended that irrigants such as sterile saline or 0.2–2% chlorhexidine gluconate are used.14,15,16
Conclusion
This case highlights the potentially hazardous complications of NaOCl incidents, their clinical presentation and the importance of early recognition and management by an appropriate MDT. It is imperative that clinicians are aware of the clinical presentation of a NaOCl incident and have a system in place to review patients who may be experiencing a suspected NaOCl extrusion. Although rare, these incidents can lead to airway compromise, paraesthesia and widespread tissue necrosis. As such, it is strongly advised that appropriate precautions are in place when using NaOCl to minimize the risk of NaOCl extrusion. This ensures that both clinicians and patients are informed of the risks of using NaOCl as an irrigant during extirpation, allowing both informed consent and appropriate managements of NaOCl incidents should they occur.