Asadi-Pooya AA, Emami M, Sperling MR Age of onset in idiopathic (genetic) generalized epilepsies: clinical and EEG findings in various age groups. Seizure. 2012; 21:417-421 https://doi.org/10.1016/j.seizure.2012.04.004
National Institute for Health and Care Excellence. Epilepsies in children, young people and adults. 2025. https://www.nice.org.uk/guidance/ng217 (accessed February 2025)
Balamurugan E, Aggarwal M, Lamba A, Dang N, Tripathi M Perceived trigger factors of seizures in persons with epilepsy. Seizure. 2013; 22:743-747 https://doi.org/10.1016/j.seizure.2013.05.018
González HFJ, Yengo-Kahn A, Englot DJ Vagus nerve stimulation for the treatment of epilepsy. Neurosurg Clin N Am. 2019; 30:219-230 https://doi.org/10.1016/j.nec.2018.12.005
National Institute for Health and Care Excellence. Cannabis-based medicinal products. NG144. 2025. https://www.nice.org.uk/guidance/ng144 (accessed February 2025)
Urolagin SS, Swaroop D, Agrawal C, Dholakia Karalwad MB Management of phenytoin-induced gingival enlargement in a patient with antiphospholipid antibody syndrome: a rare case report. J Indian Soc Periodontol. 2016; 20:561-564 https://doi.org/10.4103/0972-124X.201693
Corrêa JD, Queiroz-Junior CM, Costa JE, Teixeira AL, Silva TA Phenytoin-induced gingival overgrowth: a review of the molecular, immune, and inflammatory features. ISRN Dentistry. 2011; 2011 https://doi.org/10.5402/2011/497850
Candotto V, Pezzetti F, Baj A Phenytoin and gingival mucosa: a molecular investigation. Int J Immunopathol Pharmacol. 2019; 33 https://doi.org/10.1177/2058738419828259
Károlyházy K, Kovács E, Kivovics P, Fejérdy P, Arányi Z Dental status and oral health of patients with epilepsy: an epidemiologic study. Epilepsia. 2003; 44:1103-1108 https://doi.org/10.1046/j.1528-1157.2003.04003.x
Cornacchio ALP, Burneo JG, Aragon CE The effects of antiepileptic drugs on oral health. J Can Dent Assoc. 2011; 71
Beaumont J, Chesterman J, Kellett M, Durey K Gingival overgrowth: part 1: aetiology and clinical diagnosis. Br Dent J. 2017; 222:85-91 https://doi.org/10.1038/sj.bdj.2017.71
Friedlander AH, Cummings JL Temporal lobe epilepsy: its association with psychiatric impairment and appropriate dental management. Oral Surg Oral Med Oral Pathol. 1989; 68:288-292 https://doi.org/10.1016/0030-4220(89)90213-2
Jacobsen PL, Eden O Epilepsy and the dental management of the epileptic patient. J Contemp Dent Pract. 2008; 9:54-62 https://doi.org/10.5005/jcdp-9-1-54
Bellocchio L, Inchingolo AD, Inchingolo AM Cannabinoids drugs and oral health-from recreational side-effects to medicinal purposes: a systematic review. Int J Mol Sci. 2021; 22 https://doi.org/10.3390/ijms22158329
Scully C Medical problems in dentistry, 6th edn. Edinburgh: Elsevier; 2010
Rood JP Local anaesthesia and the medically compromised patient. Dent Update. 1991; 18:330-334
Costa AL, Yasuda CL, Shibasaki W The association between periodontal disease and seizure severity in refractory epilepsy patients. Seizure. 2014; 23:227-230 https://doi.org/10.1016/j.seizure.2013.12.008
Nonato ER, Borges MA Oral and maxillofacial trauma in patients with epilepsy: prospective study based on an outpatient population. Arq Neurpsiquiatr. 2011; 69:491-495 https://doi.org/10.1590/S0004-282X2011000400016
Karolyhazy K, Kivovics P, Fejerdy P, Aranyi Z Prosthodontic status and recommended care of patients with epilepsy. J Prosthet Dent. 2005; 93:177-182 https://doi.org/10.1016/j.prosdent.2004.11.008
Gray D, Barraclough O, Ali Z, Nattress B Modern partial dentures – part 2: a review of novel metal-free materials and innovations in polymers. Br Dent J. 2021; 230:813-818 https://doi.org/10.1038/s41415-021-3068-y
King P, Foster L, Yates R, Newcombe RG, Garrett MJ Survival characteristics of 771 resin-retained bridges provided at a UK dental teaching hospital. Br Dent J. 2015; 218:423-428 https://doi.org/10.1038/sj.bdj.2015.250
Abdullah BJ, Teong LK, Mahadevan J, Jalaludin A Dental prosthesis ingested and impacted in the esophagus and orolaryngopharynx. J Otolaryngol. 1998; 27:190-194
Mawardi H, Alsubhi A, Salem N Management of medication-induced gingival hyperplasia: a systematic review. Oral Surg Oral Med Oral Pathol Oral Radiol. 2021; 131:62-72 https://doi.org/10.1016/j.oooo.2020.10.020
BSc (Hons), BDS, FDS RCPS, FCGDent, MRD RCS Ed, MClinDent, FDS RCS(Rest Dent), FDTFEd, FFD RCSI, FHEA, Head of School, Director of Clinical Dentistry, Peninsula Dental School, University of Plymouth
BDS(Hons), FDS RCS(Eng), DSCD RCS(Eng), PGDip Clin Ed, FHEA, Consultant in Special Care Dentistry, King's College Hospital NHS Foundation Trust, London
Epilepsy is a common neurological condition that affects approximately 630,000 people in the UK. It is caused by disordered bursts of electrical activity in the brain, which affect the way it works. It is an often-misunderstood condition, with many dental professionals assuming patients with epilepsy have exclusively tonic-clonic seizures. There are two groups of seizures: generalized and focal, with multiple types within those categories. Every dental practice will have patients with epilepsy, and it is imperative to know how to manage each of the types of seizures if one were to happen in the dental chair. Patients with epilepsy are likely to be on at least one drug that can have oral side effects, which can increase risks of caries and periodontal disease. It is thus important that dental team members are cognizant of the complications associated with these drugs in order to optimise patient care.
CPD/Clinical Relevance: Dental professionals should be aware of different types of seizures, know what questions to ask patients with epilepsy and know the relevance to treatment planning.
Article
Epilepsy is one of the most common neurological conditions worldwide with approximately 630,000 people living with epilepsy in the UK and approximately 80 new diagnoses made every day.1 It is caused by disordered bursts of electrical activity in the brain, which affect the way the brain functions.
Despite its frequency, the presentation of epilepsy is often misunderstood, with the focus on patients having tonic-clonic or, as previously known, grand-mal seizures, often referred to as fits. Although our understanding of epilepsy is often based around patients having tonic-clonic seizures, there are several different types of seizures, which are divided into two broad categories: generalized and focal.2
Epilepsy symptoms begin in childhood 75% of the time, most commonly before adolescence.3,4 People with learning disabilities are more likely to have epilepsy, with around 32% of people with a mild–moderate learning disability having the condition; 20% of those with epilepsy have a learning disability.5
When epilepsy is diagnosed in later life, the patient is likely to be aged >60 years and the cause is most likely to be secondary to another neurological disorder, such as Alzheimer's, stroke or following head injuries or surgeries.6
Types of seizures
There are two groups of seizures: generalized and focal. Within these are many subtypes with different presentations.
Generalized seizures occur when both sides of the brain are affected and consciousness is always lost, even if only for a very brief period. Focal seizures, however, start in one part of the brain with the possibility of spreading. There are more than 40 types of seizure, with the most common types mentioned within this article. This is why it is importance of recording a detailed seizure history from each patient. Table 1 gives a summary of some epileptic seizure types.
The patient remains conscious, but can appear dazed and may carry out actions of which they are unaware. These seizures usually last up to a couple of minutes but can go on for longer periods of time
Either twitching of a body part or a change in sensation occurs, such as feeling frightened, déjà vu or a rising sensation in the stomach These are often referred to as auras when they progress to generalized (secondary generalized seizure/focal to bilateral tonic-clonic seizure) or focal impaired awareness seizures
Auras
Some patients experience a warning sign that a seizure is coming, known as an aura. The presentation of an aura can vary between patients. They can range from visual disturbances to déjá vu and unpleasant tastes and smells.8,9
The presence of auras in those with focal-to-bilateral tonic-clonic seizures can be extremely helpful as they may provide a short period of time to access a safe place or position where their usual seizure can occur. This, however, cannot always be relied upon because the aura may occur a split second before progression to a generalized seizure.
It is therefore imperative that a patient is told to inform the clinician at the start of the appointment if they have an aura, as it gives the dental team time to move the patient into a safe position.
Non-epileptic seizures
Non-epileptic seizures are episodes that appear like epileptic seizures but do not involve abnormal electrical brain activity. There are two causes of non-epileptic seizures: organic and psychological (often referred to as dissociative seizures).
Non-epileptic seizures may have a physical/organic cause (e.g. hypoglycaemia) or may be related to heart function. These types are easier to treat than those where the aetiology is psychological. Organic causes of seizures can be treated with medication whereas the treatment for dissociative seizures will be most likely to consist of talking therapies and/or antidepressant drugs if the patient also has anxiety or depression.10
First Aid
Tonic-clonic seizures
A tonic-clonic seizure is often the most recognized type because it involves excessive movements. To provide basic first aid for tonic-clonic seizures, the acronym CARE can be used: comfort, action, reassure, emergency (Table 2).11
Comfort
Protect the patient's head with something soft, e.g. the patient's rolled-up jacket or a pillow/cushion that is present in the surgery
Action
Clear the area of anything that is harmful. This would include the spittoon, bracket table and anything sharp such as burs and needles. If the patient is the waiting room, clear away any chairs
Make a note of the time that the seizure started
Call for help
Complete an ABCDE (airway, breathing, circulation, disability, exposure) assessment
Review the medical history to remind yourself of the patient's seizure history
Reassure
After the seizure, place the patient into the recovery position. Stay with the patient and comfort them as they start to regain consciousness. Administer oxygen at 15 l/min
Emergency
If the seizure lasts for >5 minutes, or the patient goes straight into another seizure, it is called status epilepticus
Status epilepticus
If a tonic-clonic seizure is prolonged and lasts for more than 5 minutes, it is referred to as status epilepticus.12,13
The recommended drug for status epilepticus in the dental setting is midazolam, delivered as a gel via the buccal sulcus. These can come in pre-filled or syringes or self-fill syringes can be used. Pre-filled is recommended to ensure the correct dose is given accurately and quickly.
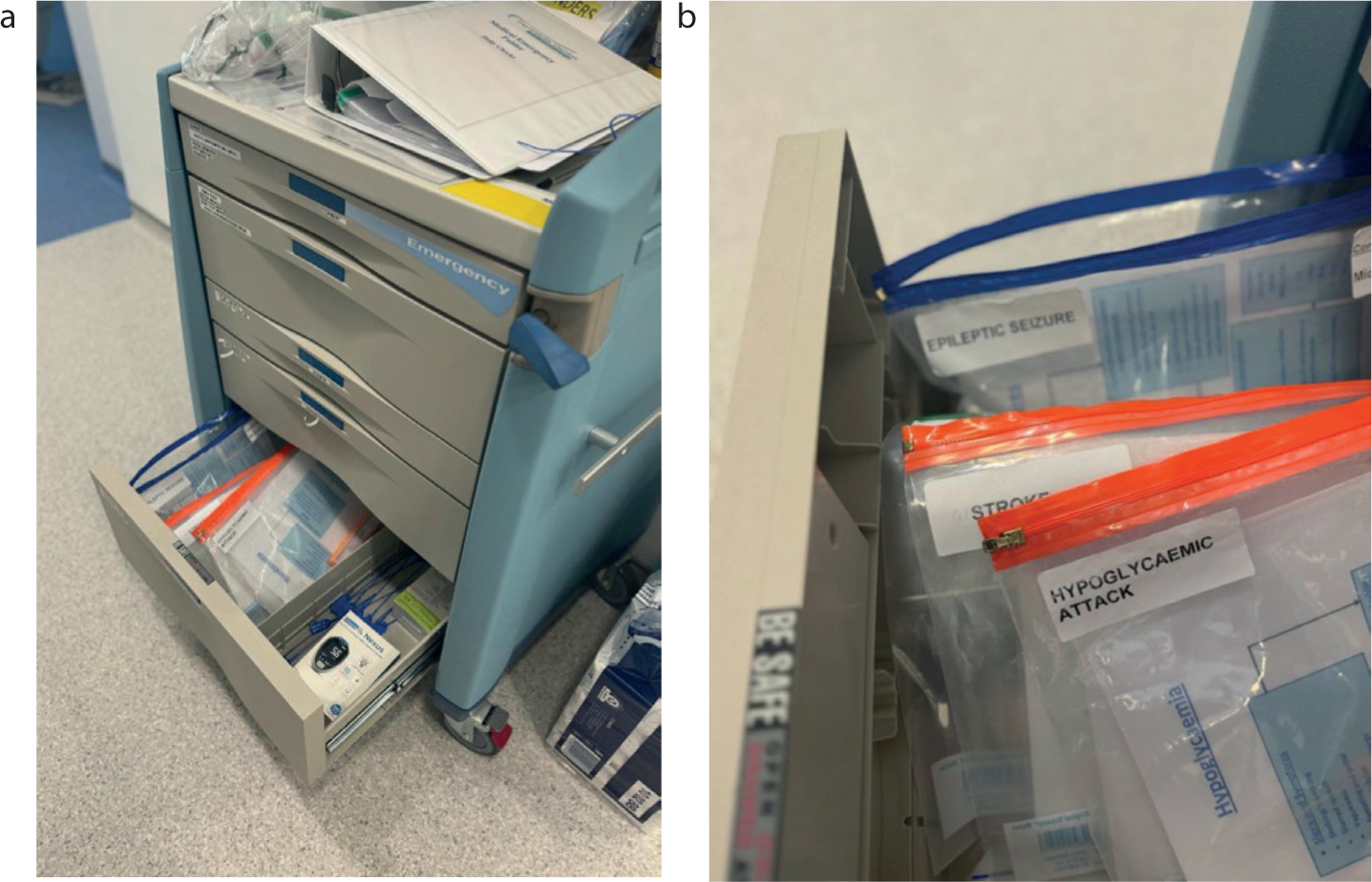
Buccal midazolam should be stocked in the medical emergency trolleys/kits in all practices (Figure 1). If a patient has a history of status epilepticus, it is likely that they will have their own supply of buccal midazolam that can be used as first-line treatment.
Figure 1. (a,b) Medical emergency trolley with emergency-specific pouches
Buccal midazolam is licensed only for use in paediatric patients, but is routinely used off label for adults. If a patient is in status epilepticus, an ambulance should called stating ‘status epilepticus’ along with your location and any other relevant details. Table 3 shows doses of buccal midazolam by age range.
Age range
Midazolam (mg)
6–11 months
2.5
1–4 years
5
5–9 years
7.5
10+ years
10
Acute repetitive seizures
In this situation, the patient comes out of a seizure and then rapidly starts another, sometimes without recovering in between.16 The management should be the same as for status epilepticus, including calling an ambulance.15
Other seizure types
The main priority when someone is having a seizure is to make the area safe. In the dental practice, this can include:
Laying the chair into the emergency position if the seizure occurs in the surgery (low to the ground);
Move away the bracket table and any sharp objects nearby;
If a patient has a seizure in the waiting room, move any tables or chairs around them out of the way.
If the patient has a seizure plan, it must be followed during and after the seizure. Once the seizure has completed, inform the patient you believe they have had a seizure and ask if there is anything you can do for them. An ambulance does not need to be called for every seizure. The situations where one needs to be called include when:
The seizure lasts longer than usual for the patient;
It has been more than a year since their last seizure;
If the patient has injured themselves (e.g. head or neck trauma);
Buccal midazolam has been provided.
Treatment and examinations can also continue if the patient consents and if there is no need for an ambulance to be called.11
If a patient starts to have a seizure, but no previous seizures are reported in their medical history, an ambulance should be called as the cause of the seizure is unknown.
Triggers
Seizures can be caused by anything that disrupts the normal connections between nerve cells in the brain. Seizure triggers are things that can make seizures more likely for some patients with epilepsy, and many have been reported over the years.
The most well-known one is the photosensitive (flashing light) trigger; however, it affects only around 3% of patients with epilepsy in the UK.17 Other triggers that have been reported are emotional stress, fatigue, sleep deprivation, missing meals, pain, excitement or shock. Dental practitioners must be mindful when treating anxious patients or patients attending for emergency appointments because, in these situations, a seizure could be triggered in the dental chair.18
One of the commonest seizure triggers is missing medication, so it is wise to ask and ensure at the start of appointments that the patient has taken their anti-seizure medication(s) as normal. It is also recommended to check that the patient is not excessively tired and has eaten as normal.19
There have been rare reports of seizures being triggered by toothbrushing. It must be emphasized that this is extremely rare. It has been reported for manual (when brushing vigorously for more than the recommend time frame) and electric-powered toothbrushes (where abnormal brain activity has been shown on an electroencephalogram).20
Treatment of epilepsy
The first-line treatment for epilepsy is anti-seizure medication (ASMs), which include lamotrigine, levetiracetam, sodium valproate and carbamazepine, among others.8
Other forms of treating epilepsy include vagal nerve stimulation (VNS) and brain surgery. These are more commonly used when at least two ASMs have been attempted and have been unsuccessful; the condition here is often referred to as refractory or drug-resistant epilepsy.21,22
VNS includes the insertion of a generator into the chest under the skin with a lead attached to the left vagus nerve. The generator sends regular pulses of electricity to the brain, which can help reduce the number of seizures. Patients who have an aura can also pass a specific magnet over the generator to send an extra pulse that may stop the seizure or decrease its severity. It can also be used by people around the patient during a seizure to help stop the seizure or reduce its severity. One dental effect of a VNS device is that, when stimulated, it can cause jaw or tooth pain. If this is significantly impacting a patient's quality of life, suggest that they speak to their epilepsy team for advice.
Cannabinoids are also used in the treatment of epilepsy. They are predominantly used for the treatment of a genetic form of severe epilepsy (Lennox–Gastaut syndrome) and also for Dravet syndrome. These can be prescribed under the instruction of a neurologist.23
Table 4 lists drugs prescribed for different types of seizures.
Medications
Seizure type
Lamotrigine
Focal and generalized
Levetiracetam
Focal with or without secondary generalization
Lacosamide
Focal with or without secondary generalization
Sodium valproate
Focal and generalized
Cenobamate
Focal with or without secondary generalization
Cannibidiol
Specific epilepsy syndromes
Zonisamide
Focal with or without secondary generalization
Brivaracetam
Focal with or without secondary generalization
Carbamazepine
Focal and generalized
Phenytoin
Focal and generalized tonic-clonic
Topiramate
Focal and generalized
Seizure history taking
The following should be included when taking a seizure history:
The type/s of seizure experienced. Ask the patient to describe their seizure;
Any known triggers?
Is an aura experienced?
If an aura is experienced, does it always progress into a seizure and, if it does, how long does it usually take to start?
How well controlled is their epilepsy? Include the date of last seizure and usual frequency (e.g. do their seizures come in clusters?);
How long does the seizure normally last, including whether there have been any episodes of status epilepticus?
Do they have any rescue medications such as buccal midazolam?
If the patient has a VNS device, do they have the magnet on them and how does it work?
How do they like to be cared for after a seizure?19,24
Oral side effects of anti-seizure medication
Medications are the first line of treatment for epilepsy, and many of them have a variety of side effects including some that affect the oral cavity.8
Gingival hyperplasia (GH) has been linked to phenytoin, with poor oral hygiene having a significant effect on the severity.23,25,26 GH arises at least 1 month after the start of any treatment and can take 1–6 months to resolve after the drug has been stopped.19,27 Other drugs, such as sodium valproate and carbamazepine, have shown GH as a side effect, but it is less common and not as severe when present.28,29,30,31
One of the most common side effects of all drugs is xerostomia, which has been reported for lamotrigine, carbamazepine and lacosamide.23
As well as GH, sodium valproate has many other possible oral side effects including xerostomia, stomatitis, dysgeusia and glossitis.23,32 This can lead to discomfort for the patient and increases the likelihood of caries.
If any of these side effects are having a significant impact on the patient's oral health or quality of life, you or the patient should contact their epilepsy specialist nurse (ESN) or neurologist.
Cannabinoids also have been shown to affect oral health.23 One side effect is dry mouth. The literature reports conflicting results with regards to the periodontal effects. Some studies have shown alveolar bone loss and GH to be side effects of cannabinoids.33
Considerations when prescribing
When prescribing medications, it is good practice to check for any interactions through the British National Formulary website or app, especially for patients with complex medical histories. There are certain medications in the Dental Practitioners' Formulary that can increase the effectiveness of certain ASMs, which can lead to overdose:
Aspirin with sodium valproate can increase tendency to bleed;
Azole antifungals can interact with both phenytoin and carbamazepine, and also increase the tendency of bleeding with sodium valproate;
Metronidazole can interact with phenytoin and increase the tendency of bleeding with sodium valproate.34
The pharmacological activity of two drugs can be changed by anticonvulsants: paracetamol, where hepatoxicity could be increased; and doxycycline, where metabolism may be increased.23
There have been reports of lidocaine being contraindicated for those with epilepsy, but this is more of a concern if it is being administered intravenously. It is believed to be safe as long as standard local anaesthetic techniques are followed and doses do not exceed the maximum recommended amount.24,35
Dental effects of epilepsy
Tooth surface loss
Patients having one or more tonic-clonic seizures per year have been shown to have abrasion in the lower arch.28 Many patients with epilepsy, even if it is controlled, have an increased risk of severe bruxism.28,29
Periodontal disease and caries
In addition to the increased risk of periodontal disease and caries from the side effects of ASMs, there is also a significant relationship between epilepsy and periodontal disease and caries.28,29 A cross-sectional epidemiological study has shown that these patients have a higher DMFT index score in comparison to a control group whether the cause is periodontal disease, caries or trauma.28 Another cross-sectional study has shown a relationship between the severity of seizures and a poorer periodontal prognosis.36
Oral trauma
Seizures can cause oral trauma to both the soft and hard tissues.28
During tonic-clonic and tonic seizures, there is often clenching of the jaw that can lead to lacerations to the tongue and buccal mucosa.37,38 Hard-tissue trauma can be in the form of tooth fracture, luxation injuries and avulsion.
Along with these intra-oral injuries, there are chances of injury to the mandible and temporomandibular joint.39
Dental management
Prevention
Prevention is key to all aspects of healthcare as it saves patients going through sometimes long and stressful appointments.
Patients with epilepsy have been shown to be more at risk for both periodontal disease and caries. It is imperative that individual caries/periodontal risk assessments are carried out to determine the appropriate treatment pathway and recall periods for each patient.
Preventive measures should be instituted in accordance with guidance from the Delivering better oral health toolkit (DBOH), which is included in Table 5.40
Advice
Professional intervention
Brush twice a day: once just before bed and at one other time
Apply 2.26% fluoride varnish twice or more a year (twice a year for adults)
Spit the toothpaste out and do not rinse after
For those aged ≥8 years, prescribe a 0.05% fluoride daily mouth rinse to use at a different time to brushing if they have active caries
Supervised or assisted brushing if required
For those aged ≥10 years with active caries, prescribe 2800ppm toothpaste
Minimize amount and frequency of sugary foods and drinks
For those aged ≥16 years or above with active caries, prescribe 5000ppm toothpaste
Use a 0.05% fluoride daily mouth rinse at a different time to brushing
Liaise with the patient's GP to see whether any medications that contain sugar can be changed to a sugar-free alternative
Assign a shortened recall of between 3 and 12 months
Soft dental splints/mouth guards
It is advised that people who experience tonic-clonic/tonic seizures should not wear soft splints because of the risk of them breaking, with the resulting smaller, loose fractured sections posing a risk to the airway.41
However, if a patient does not experience tonic-clonic seizures, the provision of a soft splint/mouthguard may be advisable if it could be of benefit. In this instance, it would still be wise to contact the patient's ESN or neurologist for their opinion.
Orthodontic aligners and retainers
The number of patients opting for orthodontic aligners over fixed appliances is increasing. For patients who have epilepsy, these can be deemed safe; the short period of time each aligner is being worn means it is unlikely to be worn through.
If a patient's epilepsy is severe, with multiple tonic/tonic-clonic seizures a day, it should be questioned whether aligners would be safe and the patient's neurology team should be consulted before any treatment is started.
For retainers, it is recommended to have fixed over removable retainers because the patient may have seizures during the night and, if retainers are displaced, this would lead to a risk of aspiration. If the patient has auras, advise them to take the aligner/retainer out before the seizure starts.
Removable appliances for tooth replacement
The majority of patients living with epilepsy have their condition well controlled and, if a patient has not had a seizure for 1 year, they are considered safe to drive.42,43 It is therefore reasonable to say it is safe for removable prosthodontic appliances to be provided to such patients.42
However, where epilepsy is poorly controlled, it would be deemed safest to have a fixed prosthetic option, e.g. implants.41,44 When a fixed prosthesis is not possible and where removable partial dentures are needed, cobalt–chrome is the gold standard, owing to its greater strength and improved retention thanks to its strict path of insertion and removal.19
After providing the patient with a removable appliance, inform them that they should remove it if they have an aura; enough force could be applied during a seizure to cause the cobalt–chrome clasps to fracture, which would pose a risk to their airway.45
Adding a metal extension from the back of pontic teeth extending onto the palate would help strengthen the denture.
For complete dentures, cobalt–chrome can be used to support the acrylic going over the alveolar ridges, but should not be extended to the post-dam area to make any adjustments required easier to carry out.19
Resin-bonded bridges
The largest cause of resin-bonded bridge (RBB) failure is debonding of the bridge from the abutment and is most likely to happen in the first 4 years of placement.46,47
If an RBB were to fail when a patient was having a seizure while unconscious, there is a risk of airway obstruction. One of the ideal conditions for RBBs is for the patient to have no parafunctional habits and, if a patient is having tonic or tonic-clonic seizures, it is likely that an unusual level of force will be applied to the dentition, because the muscles uncontrollably contract, therefore increasing chance of failure at the time of seizure.48
Treatment of caries and periodontal disease
Carious lesions would ideally be restored with materials such as composite owing to it satsifactory compressive strength and its ability to bond to the tooth, decreasing the chance of fracture.49 It is highly resistant to abrasion and attrition.
Indirect ceramic inlays and the replacement of cusps are contraindicated for patients with epilepsy owing to the risk of fracture and subsequent aspiration of pieces.28,50 A mouth prop is advisable when undertaking treatment to allow for safe removal of dental instruments should a seizure start, which then can be removed once everything else is out of the patient's mouth.19
Treatment of periodontal disease should remain as standard in most cases as per British Society of Periodontology guidelines. Optimizing oral hygiene is as always key and, as inflammation is a key driver for gingival hyperplasia, reinforcement of oral hygiene and regular maintenance appointments are essential for patients with GH.
Where GH is present, there are two strategies: surgical and non-surgical management. Initially, the most successful treatment, which is non-surgical, is the cessation of the drug causing the overgrowth. This needs to be carried out by contacting the patient's ESN, neurologist or GP; however, if the seizures are well controlled, an alteration of the medication is unlikely.
Surgically, there are two methods: excision of hyperplastic gingivae and laser resection. Excision of hyperplastic gingiva requires a referral to a specialist periodontist and has good success rates. Laser resection can be completed by restorative dentists and oral surgeons.51 However, gingival overgrowth is likely to re-occur if the medication is not changed and oral hygiene is not optimized.
Non-surgically, folic acid supplements along with non-surgical periodontal treatments and effective oral hygiene are important.52
Oral trauma
Patients with soft tissue trauma are likely to present directly to the emergency department. However, they may also attend in primary care. You should check that there have been no secondary seizures and the patient did not injure their head. Sutures are not always necessary but, if a laceration is >1 cm, they could be justified, especially if there is uncontrolled bleeding.53
For hard tissue injuries, the international dental trauma guidelines should be followed (https://www.iadtdentaltrauma.org/bkk/for-professionals.html). This is with the exception of avulsion, where it is deemed inappropriate to replant the tooth.19
When to refer
Epilepsy is one of the most common neurological disorders and general dental practitioners should be prepared to treat patients who experience seizures, taking into account the advice and recommendations in this article.
However, where there are complexities, referral to special care dentistry should be considered. Complexities include if the patient still has seizures (their epilepsy is uncontrolled) and:
They have a severe learning disability;
They have several tonic/tonic-clonic seizures per week;
They cannot tolerate treatment under local anaesthesia;
You feel you are not equipped to manage their needs.54
Special care dentistry teams will have alternative treatments available to them that can help prevent seizures. These treatments can include both inhalation and intravenous conscious sedation along with general anaesthesia. Intravenous sedation techniques can be particularly helpful to induce seizure suppression and therefore allow safe patient treatment.
Conclusion
Epilepsy is a complex neurological condition that affects many people, and has a wide spectrum of presentations. This needs to be considered when treating any patients who have the condition. It is critical to know how epilepsy affects each patient sitting in the chair so, if a seizure were to happen, all the team are prepared.
Taking an appropriate seizure history is of key importance in managing such patients. Dental visits can of course be stressful, and stress is a known trigger for seizures. Understanding the patient's condition and tailoring the appointment to the specific patient will help limit this stress for all concerned as far as possible.