Ward LM, Cooper SA, Hughes-McCormack L Oral health of adults with intellectual disabilities: a systematic review. J Intellect Disabil Res. 2019; 63:1359-1378 https://doi.org/10.1111/jir.12632
Morgan JP, Minihan PM, Stark PC The oral health status of 4,732 adults with intellectual and developmental disabilities. J Am Dent Assoc. 2012; 143:838-846 https://doi.org/10.14219/jada.archive.2012.0288
Cumella S, Ransford N, Lyons J, Burnham H Needs for oral care among people with intellectual disability not in contact with Community Dental Services. J Intellect Disabil Res. 2000; 44:45-52 https://doi.org/10.1046/j.1365-2788.2000.00252.x
Byrappagari D, Jung Y, Chen K Oral health care for patients with developmental disabilities: a survey of Michigan general dentists. Spec Care Dentist. 2018; 38:281-290 https://doi.org/10.1111/scd.12303
Lees C, Poole H, Brennan M, Irvine F Adults with learning disabilities experiences of using community dental services: service user and carer perspectives. Br J Learning Disabilities. 2017; 45:114-120
Gordon SM, Dionne RA, Snyder J Dental fear and anxiety as a barrier to accessing oral health care among patients with special health care needs. Spec Care Dentist. 1998; 18:88-92 https://doi.org/10.1111/j.1754-4505.1998.tb00910.x
McGeown D, Stapleton S, Nunn J A cost analysis estimation of a single episode of comprehensive dental treatment under general anaesthesia for adults with disabilities. Br Dent J. 2018; 224:442-446 https://doi.org/10.1038/sj.bdj.2018.124
Phadraig CMG, Griffiths C, McCallion P Communication-based behaviour support for adults with intellectual disabilities receiving dental care: a focus group study exploring dentists' decision-making and communication. J Intellect Disabil. 2019; 23:526-540 https://doi.org/10.1177/1744629517738404
MacGiolla Phadraig C, Asimakopoulou K, Daly B Nonpharmacological techniques to support patients with intellectual developmental disorders to receive dental treatment: a systematic review of behavior change techniques. Spec Care Dentist. 2020; 40:10-25 https://doi.org/10.1111/scd.12434
Mac Giolla Phadraig C, Newton T, Daly B BeSiDe time to move behavior support in dentistry from an art to a science: a position paper from the BeSiDe (Behavior Support in Dentistry) Group. Spec Care Dentist. 2022; 42:28-31 https://doi.org/10.1111/scd.12634
Bradshaw J The use of augmentative and alternative communication apps for the iPad, iPod and iPhone: an overview of recent developments. Tizard Learning Disability Review. 2013;
Samuels R, Stansfield J The effectiveness of social stories™ to develop social interactions with adults with characteristics of autism spectrum disorder. Br J Learning Disabilities. 2012; 40:272-285
Richardson PH, Black NJ, Justins DM, Watson RJ The use of stop signals to reduce the pain and distress of patients undergoing a stressful medical procedure: an exploratory clinical study. Br J Med Psychol. 1999; 72:397-405 https://doi.org/10.1348/000711299160086
Greenbaum PE, Turner C, Cook EW, Melamed BG Dentists' voice control: effects on children's disruptive and affective behavior. Health Psychol. 1990; 9:546-558 https://doi.org/10.1037//0278-6133.9.5.546
de Castro AM, de Oliveira FS, de Paiva Novaes MS, Araújo Ferreira DC Behavior guidance techniques in pediatric dentistry: attitudes of parents of children with disabilities and without disabilities. Spec Care Dentist. 2013; 33:213-217 https://doi.org/10.1111/scd.12022
Allen KD, Wallace DP Effectiveness of using noncontingent escape for general behavior management in a pediatric dental clinic. J Appl Behav Anal. 2013; 46:723-737 https://doi.org/10.1002/jaba.82
Altabet SC Decreasing dental resistance among individuals with severe and profound mental retardation. J Development Phys Disabilities. 2002; 14:297-305
Conyers C, Miltenberger RG, Peterson B An evaluation of in vivo desensitization and video modeling to increase compliance with dental procedures in persons with mental retardation. J Appl Behav Anal. 2004; 37:233-238 https://doi.org/10.1901/jaba.2004.37-233
Chen Y, Hawkins J Effects of music listening to reduce preprocedural dental anxiety in special needs patients. Complement Ther Clin Pract. 2021; 42 https://doi.org/10.1016/j.ctcp.2020.101279
Kritsidima M, Newton T, Asimakopoulou K The effects of lavender scent on dental patient anxiety levels: a cluster randomised-controlled trial. Community Dent Oral Epidemiol. 2010; 38:83-87 https://doi.org/10.1111/j.1600-0528.2009.00511.x
Prangnell SJ, Green K A cognitive behavioural intervention for dental anxiety for people with learning disabilities: a case study. Br J Learning Disabilities. 2008; 36:242-248
Marshman Z, Morgan A, Porritt J Protocol for a feasibility study of a self-help cognitive behavioural therapy resource for the reduction of dental anxiety in young people. Pilot Feasibility Stud. 2016; 2 https://doi.org/10.1186/s40814-016-0054-2
Patient-support techniques for treating patients with learning disabilities Stephanie Fenesan Jennifer Hare Bryan Kerr Dental Update 2025 51:2, 122-130.
Authors
StephanieFenesan
BDS, BSc(Hons), AKC, MSc, MSCD RCS Ed
Specialty Trainee in Special Care Dentistry, Department of Sedation and Special Care Dentistry, Guy's Dental Institute, Guys and St Thomas' NHS Foundation Trust
Consultant in Special Care Dentistry, Department of Sedation and Special Care Dentistry, Guy's Dental Institute, Guys and St Thomas' NHS Foundation Trust, London
There are many techniques that can, with simple adjustments, be used for patients with learning disabilities. A number of techniques may be familiar to dentists as those which are applied to anxious or paediatrics patients. There is a lack of focused articles clearly describing specific techniques that can be used for individuals with learning disabilities and how these can be adapted to help enable dental assessment and treatment. This article aims to inform general dental practitioners of patient-support techniques that may be used or adapted for individuals with learning disabilities.
CPD/Clinical Relevance: Dental professionals should be able to make reasonable adjustments to their practice to better support individuals with learning disabilities who access dental care.
Article
Mencap estimates that there are approximately 1.5 million people in the UK with a learning disability, affecting an estimated 2.16% of adults and 2.5% of children.1 Individuals with learning disabilities will present with a reduction in intellectual ability and difficulties with learning and understanding new information, social tasks and completing activities of daily living, resulting in the need for additional support.2 There are varying degrees of learning disabilities (LD), ranging from mild to severe/profound, which will affect the capabilities of an individual as well as their ability to communicate and understand social interaction (Table 1). Under the Equality Act (2010), organizations, including dental services, must make reasonable adjustments to ensure services are accessible for people with learning disabilities.3
Owing to difficulties with social interaction and communication, patients may require additional time to support understanding, along with adjustments in communication methods, such as using clear simple language and easy-to-read leaflets with pictures.4 The patient's capacity to consent for treatment may be affected, and capacity must be assessed according to the principles of the Mental Capacity Act.5 Adults with learning disabilities experience poorer oral health, including suboptimal oral hygiene, poor gingival health and a higher prevalence of dental caries and periodontitis.6,7 They also have higher incidence of unmet dental needs.8 This cohort of patients can find it difficult to access dental services, and when they do, dentists report difficulties in providing care, with commonly cited reasons including behaviour management of the patient and inadequate training or experience.9
There are several key barriers that individuals with LD experience when accessing dental services. These include lack of awareness among carers, as well as dental anxiety, with a reported prevalence of more than 50% and which often increases when patients feel they are not listened to.2,8,10,11 Patients with learning disabilities may experience difficulties in communicating their anxieties effectively and this may manifest as behaviours that challenge clinicians, such as running away, ‘hitting out’ or other inappropriate actions.
The options for supporting for these patients to access dental care include pharmacological patient-support techniques (PSTs), such as conscious sedation or general anaesthetic (GA) and non-pharmacological PSTs. The use of the latter may aid in reducing the need for pharmacological interventions, which can be advantageous in improving access to routine dentistry in primary care. Additionally, there are cost implications of providing treatment with conscious sedation or GA, and often the range of treatment offered may be limited.12,13
Patient-support techniques
Historically these techniques have been referred to as non-pharmacological behaviour management techniques, although they have recently been appropriately termed ‘non-pharmacological patient-support techniques’.14
In a systematic review of PSTs for patients with learning disabilities having dental treatment, there was evidence of improvements in outcomes, although there was limited evidence to support effectiveness of any one technique in particular.14
In this article, the present authors acknowledge that the lack of standardized terminology presents a problem to the ongoing discussions around this topic. Taking the time to address this, and develop some universally agreed terminology is an area that has been identified as requiring further research.15 Nonetheless, this article will adopt the broad terms advocated in the seminal paper by Phadraig et al with a focus on the practical application of PSTs within the broad categories of: communication, reinforcement, modelling, desensitization, distraction/relaxation and, adapting the clinical environment.14
This article describes PSTs that can be appropriately used for individuals who have learning disabilities within primary care, and how they can be adjusted to optimise their use based on practical clinical experience. Use of physical restrictive methods, such as clinical holding, will not be covered as this is outside the scope of this article.
Communication
Communication aids can be used during appointments to facilitate communication and include the use of pictures boards, social stories and Makaton flash cards, among other methods, including the use of technology on tablet and smart phones to aid with communication.16 It is important for an individual to attend with a family member or carer who can assist; however, every effort should be made to engage with the patient directly, using their preferred means of communication.
Non-verbal communication is also an important aspect of communication, especially so for individuals with learning disabilities who may rely on facial expression, body language and touch to a larger extent then verbal communication.
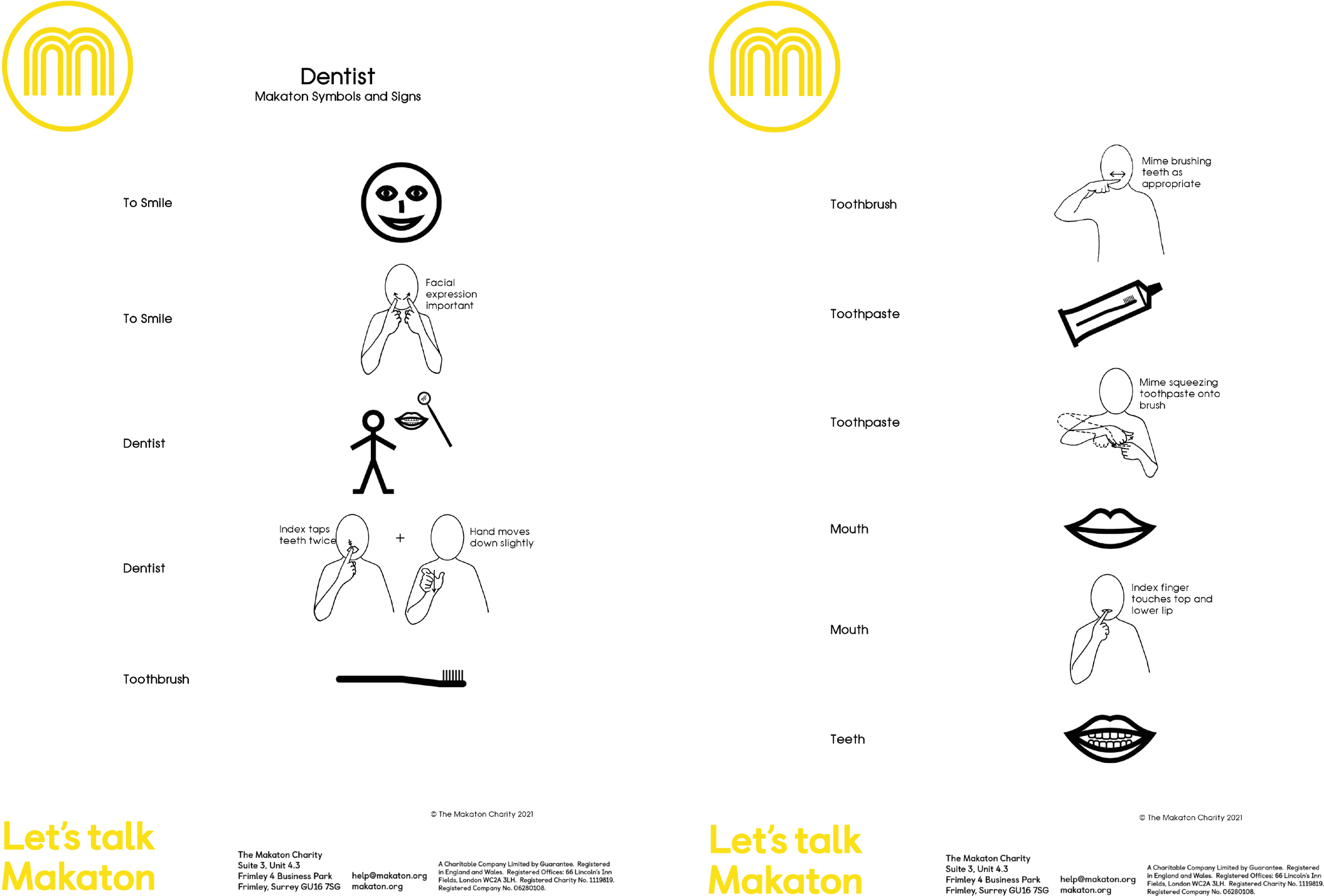
Makaton is a language programme that uses simple signs and symbols to provide a visual representation to aid with understanding and to help make communication easier (Figure 1). It is designed for people with communication difficulties, many of whom include those with learning difficulties (www.makaton.org). Flashcards with accompanying pictures or Makaton symbols in the dental surgery can be beneficial to help patients understand what is happening and what is expected of them during a dental visit. Makaton signs and actions specific to the dental environment are also available at the Makaton charity website.17
Figure 1. An example of Makaton signs and symbols that may be used during a dental appointment.17
An additional helpful resource is the book ‘Going to the Dentist’, which is a wordless book with plenty of pictures about visiting the dentist (Figure 2).18
Figure 2. ‘Going to the Dentist’ book.18
Preparatory information
Preparatory information commonly refers to the information given to the patient to prepare them for what to expect; however, clinician preparation is essential in helping appointments run more smoothly.
Prior to an appointment with a new patient, it is essential to find out how the person communicates and any further information about what may be helpful. This may include their level of understanding, any communication aids used, as well as previous experiences of visiting the dentist. Some patients with learning disabilities may have a ‘hospital/healthcare passport’ that provides a summary of this information.1
Preparatory information for patients, such as a social story, provided prior to appointments, can be a useful way to support patients with learning disabilities and their family/carers to prepare for dental appointments. Through the use of pictures or photographs, a social story may detail the steps involved in visiting the dentist, such as going to the waiting room, coming into the dental surgery, and using a small mirror. This can help patients to understand what to expect when they come to the dentist and prepare them for surroundings that may be unfamiliar. It can also help patients to become familiar with behaviours expected during dental visits. All of which can help to reduce anxiety and have a positive effect on behaviour.19
Rapport building and establishing a relationship with the patient is essential to increase cooperation.20 It is important to treat each patient as an individual and get to know their idiosyncrasies. Family members and carers who know the patient well can assist with this. Seeing the same clinician and dental assistant can help with making the patient feel more at ease and will also become familiar with how the patient best communicates and responds to situations, as well as being familiar with which techniques may have been successful previously or not.
Control involves giving the patient an element of control, which can help to reduce their anxiety.21 The use of ‘STOP’ signals' is a common example, where a patient raises their hand if they want a break or the procedure to stop. Another example is giving the patient a mirror so they can see what is happening. An additional adjustment for patients with learning disabilities may be to hold the hand of a family member or carer and to squeeze their hand who will then communicate with the clinician to stop. This can be demonstrated and practised with the patient prior to starting treatment to aid with understanding and help improve their confidence.
Tell-show-do is a widely used technique, particularly in paediatric dentistry and with anxious patients. First, an explanation of the procedure is carried out using language appropriate to the patient's level of understanding, followed by showing the procedure to the patient, such as demonstrating the slow hand piece on a patient's finger, followed by doing the action on the patient. For a patient with a learning disability with limited communication skills, the emphasis may be on demonstrating the action, rather than on describing the detail, depending on their level of understanding. Adapting the language used to describe dental equipment, similar to terms used within paediatric dentistry can also be beneficial, such as using the term ‘buzzy bee’ for the slow hand piece and ‘puff of wind’ for the 3:1. Additionally, it may help to add extra steps when ‘showing’ the patient; an example, when introducing suction, to ‘tell’ the patient what it does, to ‘show’ the patient what it does outside of the mouth (i.e. using the suction tip in a cup of water so they can see and hear the noise of the suction tip in use, then ‘showing’ the patient on their hand, then their cheek, asking them to stick out their tongue and then inside their mouth) progressively getting closer to their mouth. Additional time may be required for patients with learning disabilities and this may need to be repeated at each appointment.
Voice control involves altering the volume, tone or pace of voice to influence and direct a patient's behaviour. This can help to improve attention and compliance as well as establishing authority. An example of this can be an abrupt change from soft to loud speaking to gain attention from a patient who is not complying. It is important that the instruction is not given in anger, or to make the patient feel shamed. It should be a clear and direct instruction of what the next step you are asking them to do.22,23 This should be discussed with family members or carers prior to the appointment to avoid any misunderstandings. The levels of communication or understanding of the patient should be assessed appropriately before carrying this out.
Reinforcement
Positive reinforcement involves rewarding the patient when they display a desired behaviour, and so increasing the likelihood of a desired behaviour being repeated. This PST can be used in conjunction with a social story by incorporating rewards within the social story so that the patient has a clear idea of the steps expected, and what their chosen reward will be. Positive reinforcement may consist of both verbal and non-verbal reinforcement, as well as material rewards for positive behaviour, such as stickers or social rewards (i.e. a visit to a favourite place or time spent with a favourite person). Individual's choice/selection of the material reward is most important.24 Non-verbal reinforcement includes the use of facial expression and tone of voice, for example, responding to a desired action with a warm smile to encourage this behaviour. Verbal positive reinforcement includes the use of praise for a certain behaviour, most usefully for a specific behaviour rather than generic praise. For example, instead of saying ‘you've been very good today’, an alternative would be ‘you were very good sitting in the dental chair and having a mirror in your mouth’.
Table 1. Assessment of learning disability and suggestions for suitable interventions.1,4
Category of learning disability
Characteristics
Questions for the clinician to consider when assessing patients with learning disabilities
Suitable interventions
Mild learning disability or people with low support needs (IQ of 50–70)
May need additional time to learn new facts May need assistance with some tasks of daily living, such as cooking, taking medications, using public transport
Do they need assistance with daily tasks? Do they live independently? Do they respond to questions appropriately?
Distraction Social story Acclimatization Familiarization Desensitization Control Tell-show-do Communication aids Modelling Memory reconstruction Rapport building Adaptation of clinical environment
Moderate learning disability or people with medium support needs (IQ of 35–49)
May need assistance or support with tasks of daily living, such as cooking, taking medications, using public transport May use communication aids, such as Makaton
What level of support do they have? How do they communicate? Do they use communication aids? Do they respond to questions appropriately?
Distraction Social story Acclimatization Familiarization Desensitization Control Tell-show-do Communication aids Modelling Memory reconstruction Rapport building Adaptation of clinical environment
Severe learning disability or people with high support needs (IQ of 20–34)
May have limited verbal communication and/or use communication aids, such as Makaton, picture boards
Do they have 24-hour support? How do they communicate? Do they use communication aids? Do they respond to questions appropriately? Do they communicate verbally?
Communication aids Tell-show-do Modelling Memory reconstruction Rapport building Preparatory information Adaptation of clinical environment
Profound learning disability or people with high support needs (IQ less then 20)
May be non-verbal May need full time care and assistance with all activities of daily living
How do they communicate? Do they use communication aids? Do they communicate verbally?
Communication aids Tell-show-do Rapport building Preparatory information Modelling Memory reconstruction Adaptation of clinical environment
Agreed time frames, also known as contingent and non-contingent escape procedures, refer to the patient receiving regular scheduled breaks from dental treatment. An example includes the procedure stopping for 10 seconds every minute when prompted to provide brief breaks for the patient during treatment.25 This may be adapted for individuals with learning disabilities to provide a fixed amount of time for a task, for example, having a dental mirror in their mouth for 5 seconds and counting aloud, which can then be combined with receiving a reward and contributing towards reinforcing positive behaviour. This can also be used when using handpieces with the patient, counting down from 10 seconds followed by a break.
Modelling
Modelling and memory reconstruction is the process of acquiring behaviour through observation of a model, and can be useful when patients have limited experience of the dental environment. This can be demonstrated by watching another individual in person, or by watching a video. Generally, if the model is similar to the patient in age, gender and anxiety status, then it has a better effect.26 A related method, known as memory reconstruction, can be easily adapted for an individual with learning disabilities and includes taking a photograph of the patient sitting in the dental chair at the end of their appointment. This uses positive imagery of the individual that acts to remind the patient of what is expected, and that they have previously completed this successfully. This image could then be incorporated into an individualized social story for the patient to help them prepare for their next visit. It is essential to discuss the use of photography with the patient, if appropriate, or their family members or carers to ensure that appropriate consent and privacy issues for their use are confirmed.
Desensitization
Acclimatization/familiarization refers to a process of allowing the patient to become familiar with the dental environment and equipment used, for example, talking through the procedure and showing the equipment used at a separate appointment, without having to worry about the intervention itself. This may include showing the patient the suction and allowing them to hear the noise, touch it on their hand, then lip, then tongue, with the aim that this will increase the acceptability of the equipment and improve cooperation for dental care. This can also improve rapport and build a relationship with the dentist prior to the treatment.
This PST has been referred to as desensitization; however, systematic desensitization or graded exposure are specific interventions used within the delivery of cognitive behavioural therapy (CBT), in which the behavioural element inspires the use of acclimatization for those with a learning disability. If an individual with a learning disability is also dentally phobic, then CBT may be an approach to consider by appropriately trained individuals, in addition to the use of acclimatization. This technique has been shown to be more effective than pure demonstration and to improve acceptance of dental care in patients with learning disabilities.27,28 This technique is generally more useful for patients who are able to identify and communicate their fears.
Distraction/relaxation
Distraction
This can include encouraging the individual to think about or focus on something not related to the dental situation. Distractions include fiddle toys that the patient can concentrate on while undergoing treatment, as well as listening to music, having a family member or carer in the room with them and talking/engaging with them.29 Visual distractions may be helpful, such as tablets with cartoons or games for them to interact with. It is useful to engage with the patient and tailor this technique for different individuals and different situations within the dental setting. Video games or cartoons may also be provided as a reward for appropriate behaviour and used to shape the patient's behaviour.
Relaxation
Techniques for encouraging the patient to enter a state of relaxation can include playing relaxing music, or specific relaxation techniques. These include progressive muscle relaxation, breathing techniques and guided imagery, all of which create a focused state of relaxation. We would recommend exploring with the patient or family/carer what approach they may find most helpful.
Adapting the clinical environment
The dental environment may be quite daunting, with unfamiliar clinical sights and smells, which can contribute to increased anxiety. There is evidence that suggests that adapting clinical environments can reduce anxiety levels.30 This can include visual changes, such as exposure to positive images before entering the surgery or having treatment, as well as other changes, such as adapting lighting, dimming lights or having music of the patient's choosing. While it may not be practical to have dimmed lights during treatment, it may be useful to have the lights dimmed when the patient initially enters the dental surgery, or consider use of darkened protective glasses for the patient.
Adaptations to other sensory experiences, such as the smell of lavender, has also been shown to reduce anxiety for dental patients.30 Other methods may include the use of weighted blankets or pillows and the removal of mouthwash.
Timing of PST use
Preparation prior to appointments can help the patient to know what to expect and therefore reduce anxiety and aid in the appointment running more smoothly. Many of the PSTs that have been described can be used in conjunction, and their suitability for each patient must be assessed at an individual level. Some of the PSTs will require preparation before appointments (Table 2).
Table 2. Summary of PSTs, appropriateness for level of LD and when to use for a dental appointment.
Intervention
When to use in a dental appointment
Additional notes
Communication aids, e.g. Makaton cards, social story, hospital passport, Makaton symbols, picture boards
Useful to find out information about aids before visits and prepare aids for use during appointments
Can prepare in conjunction with the patient, their family member or care team and be used at home before the appointment
Preparatory information, e.g. social story
Prepare before appointment and use during appointment, reflect on use following appointment and amend as appropriate for future visits
Can prepare in conjunction with the patient, their family member or care team
Rapport building
During appointments
Aim to have the same dentist and assistant Can use a questionnaire before appointments to gain more information about patients' hobbies and interests
Control/‘STOP’ signals
During appointments
Can be useful to practise before carrying out treatment
Tell-show-do
During appointments
Can combine with familiarization/acclimatization
Voice control
During appointments
Important to discuss and agree with carers family members prior to using
Positive reinforcement or rewarding behaviour
During appointments
Rewards may be items, such as stickers, or social rewards, such as a visit to favourite restaurant
Agreed timeframes
During appointments
Can adjust time intervals according to patient response
Modelling
During appointments
Memory reconstruction
Before, during and after appointments
Take photographs during the appointment to aid in memory reconstruction to use after the appointment and prior to the next appointment
Acclimatization/familiarization
Prior to check-ups and treatment During, can be used prior to treatment appointments
May be useful to have an additional appointment prior to treatment visits
Distraction
During appointments
Can ask the patient to bring their favourite music, fiddle toy
Relaxation
Before and during appointments
Can provide guidance on relaxation techniques to use before and during treatment appointments
Adaptation of clinical environment, e.g. adjust lighting, no masks before communication, removal of pink water, sensory blanket, use of pillows and support, smell/lavender
Before, during and after appointments
Prior to appointment can find out information about likes/dislikes, e.g whether they dislike bright lights, and afte the appointment reflect on any aspects that could be changed/altered for the next visit
Cognitive behavioural therapy (CBT)
Before, during and after appointments These techniques can be used as an adjunct if the patient has dental anxiety/phobia
Liaise with practitioners who are trained in delivering CBT
At the end of each appointment, it is important to reflect and consider what was successful and unsuccessful, and what could be done differently. This can be completed with the patient/carer/family member and specific praise and positive reinforcement given. Even if the patient has not completed all aspects of the appointment, it is beneficial to note any actions, however small, that the patient successfully carried out. It is also beneficial to discuss what didn't go so well and why (i.e. is this a bad time of day for them?), was there anything in particular that scared or frightened them and what can be done about this? The ‘Message to the Dentist’ resource, set up by Living life to the Full in collaboration with Marshman et al33 has questions that can be completed after dental appointments to help with this. It may also be helpful to set targets for the next visit so that the patient/carer/family member is aware of what the expectations may be, and to set preparatory tasks to help with this.
Other approaches
Cognitive behavioural therapy
Separate to the specific PSTs outlined previously, it may be that an individual with a learning disability also experiences dental phobia, in which case, the addition of CBT may be a consideration. It is not within the scope of this article to fully outline CBT as an approach, because this intervention requires appropriate training and cannot be used as a one-off, ad hoc technique. Nevertheless, elements of CBT have inspired several of the PSTs outlined above, including acclimatization, distraction, relaxation and memory reconstruction.
The adaptation of CBT for people with a learning disability should not be excluded as a consideration. Learning disabilities fall on a continuum, and each individual should be appropriately and individually assessed. Research generally supports the adaptation of tailoring CBT for an individual with a learning disability, and while there is a paucity of research specific to dental phobia among individuals with a learning disability, a single case study outlines the success of adapting the approach.31,32
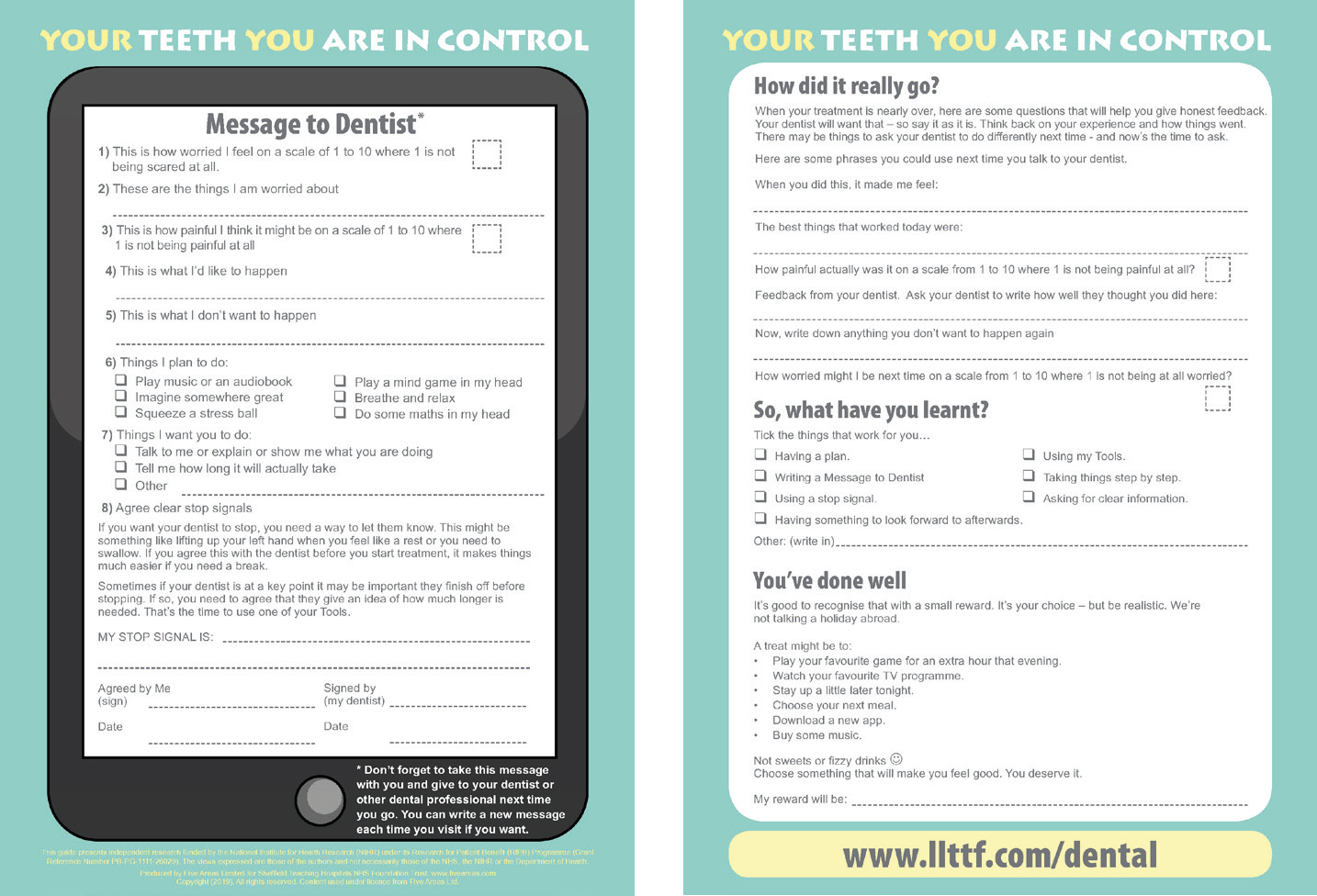
Specific CBT-based self-help documents may provide valuable resources for working with individuals with a learning disability who also experience dental anxiety/fear. Marshman et al and the Living Life to the Full team have set-up an online resource for use with young people with dental anxiety.33,34 Although not specific to individuals with a learning disability, their use may be appropriate or adapted for patients with a learning disability. Resources are highlighted in Figure 3.34
Figure 3. Message to the dentist. Dental worksheet.34 Reproduced with permission of Five Areas Ltd/Professor Chris Williams (www.llttf.com/dental).
Conclusion
It is beneficial for patients with learning disabilities to be seen in general dental practice where possible, and dental professionals should have an awareness of PSTs available to aid this. These techniques, with reasonable adjustments, may contribute to a more positive overall dental experience for patients, and increase their confidence to attend for regular visits. This assists with both building rapport with the dental team as well as providing and reinforcing regular preventive advice. Different members of the dental team can assist with the delivery of PSTs, such as preparation before appointments or acclimatization. Many PSTs may be used in combination and individual patient factors and understanding/cooperation will have a role in selecting the appropriate flexible approach, to allow the clinician to adapt their technique depending on the patient's response.