Levin L, Day PF, Hicks L International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: general introduction. Dent Traumatol. 2020; 36:309-313 https://doi.org/10.1111/edt.12574
Andreasen FM Pulpal healing after luxation injuries and root fracture in the permanent dentition. Endod Dent Traumatol. 1989; 5:111-131
Diangelis AJ, Andreasen JO, Ebeleseder KA International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 1. Fractures and luxations of permanent teeth. Dent Traumatol. 2012; 28:2-12
Andonovski ME, Antonarakis GS Autism spectrum disorder and dento-alveolar trauma: a systematic review and meta-analysis. J Stomatol Oral Maxillofac Surg. 2022; 123:e858-e864
Albadri S, Zaitoun H, Kinirons MJ UK National Clinical Guidelines in Paediatric Dentistry: treatment of traumatically intruded permanent incisor teeth in children. Int J Paediatr Dent. 2010; 20:(Suppl 1)1-2
Levin L, Day PF, Hicks L International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: general introduction. Dent Traumatol. 2020; 36:309-313 https://doi.org/10.1111/edt.12574
Treatment of Dento-alveolar Traumatic Injuries in a Child with Autism Spectrum Disorder (ASD) Afreen Osman Serena A Dodhia Kathleen Fan Meera Ahluwalia Dental Update 2025 51:9, 632-634.
This case report details the multidisciplinary management and follow-up of a 9-year-old boy diagnosed with autism spectrum disorder (ASD). He presented with severe intrusion injuries after a fall to his permanent maxillary central and lateral incisor teeth. The patient was initially seen in the emergency department by the maxillofacial team. Owing to the complexity of the dento-alveolar injury, it was felt that a multidisciplinary approach would improve patient outcomes. In theatre, both maxillofacial and paediatric dental teams managed the acute trauma. The paediatric dental team continued to review and follow-up with the child. A multidisciplinary team is ideal for managing paediatric patients with severe dental trauma and complex behavioural needs. This approach ensures the best care for patients and favourable outcomes.
CPD/Clinical Relevance: Multidisciplinary management is important in paediatric dento-alveolar trauma.
Article
Traumatic dento-alveolar injuries occur frequently in children, making up 5% of all injuries and 25% of all school children experience dento-alveolar trauma.1 Luxation injuries are the most common in the primary dentition, and crown fractures are the most commonly reported in the permanent dentition.1 Intrusion injuries have ‘an incidence of 2% of all dental trauma, with 97.2% in the anterior maxilla’.2 As a result of the force required to intrude incisors into the alveolar bone, there is typically severe damage to the periodontal ligament, root cementum, neurovascular bundle and surrounding alveolar bone.3 The damage to the supporting structures of the tooth gives intrusive luxation injuries, a comparatively worse prognosis to other types dento-alveolar injury. Some intrusive injuries can be so severe that the teeth might require extraction.
There are multiple treatment options for intrusion of maxillary upper incisors. They include monitoring to allow spontaneous eruption, immediate surgical repositioning or orthodontic extrusion. The treatment options are dependent on the severity of the intrusion and the maturity of the tooth.
For intruded permanent incisors, revitalization has a low probability, with this largely being determined by the maturity of the root and severity of the intrusion. An epidemiological study of 216 intruded permanent teeth, conducted by Andresen et al, suggested that ‘the occurrence of pulp necrosis in intruded teeth with closed apices is 100%’.2
Furthermore, there is a high risk of root resorption. Therefore, endodontic treatment is often indicated. A decision to undertake endodontic therapy can be decided early, often at the first follow-up appointment. Evidence suggests that ‘endodontic treatment of intruded teeth with closed apices should be undertaken at 2 weeks post-intrusion’.4
The patient, in this case, had been recently diagnosed with autism spectrum disorder (ASD), which can cause difficulties in behavioural management. Particularly after a trauma, a patient can be highly distressed, which will affect their co-operation. The patient's behaviour largely determines the modalities of care that can be used. This can potentially complicate the ongoing care of the child, and the ability to optimise outcome by joint care by the maxillofacial and paediatric dental teams is ideal.
Importantly, individuals with ASD have a higher prevalence of malocclusions, such as increased overjet, crowding, and anterior open bite.5 These factors may also contribute to an increased risk of dento-alveolar trauma in individuals with ASD, and are important to consider in treatment post-trauma. A meta-analysis found that individuals with ASD are at an increased risk of dento-alveolar trauma compared with those without ASD, especially for more severe dento-alveolar trauma, such as luxation and avulsion injuries.5
Case report
A 9-year-old boy presented to A&E, after falling onto a pavement while playing at school. After ensuring that the child had no head injuries or loss of consciousness, the dental injuries were addressed. The child was found to have avulsed their UR2, which was not found. Additionally, they UR1 had been intruded, UL2 had sustained an enamel dentine crown fracture, and there was lateral luxation of the UL1 with an enamel dentine crown fracture. The multitude of injuries highlighted the high impact of the fall (Figure 1).
Figure 1. Pre-operative photograph of the patient, in the operating theatre.
The patient was fit and well, with no current medications and no known allergies, but the patient had been recently diagnosed with ASD. Behaviour management was significantly more difficult, including the assessment in the emergency department. The patient was visibly very distressed by the trauma. A dental radiographic investigation could not be conducted owing to limited patient compliance. However, the patient tolerated a chest X-ray, which confirmed that the avulsed UR2 had not been aspirated.
Management could not be undertaken with local anaesthetic owing to reduced patient compliance. Following assessment and examination by the maxillofacial team, the decision was to proceed with repositioning and splinting of the affected teeth under general anaesthetic (GA). In view of the patient's age and the severity of the injury, the paediatric dental team agreed for planned joint care. Multidisciplinary management in theatre ensured a comprehensive examination of the patient.
Treatment
One day after the injury, the patient was taken to theatre, where the paediatric team carried out treatment, supported by the maxillofacial team. The UR2 was confirmed to be clinically avulsed. Management included debridement of soft tissue abrasions. The UR1, UL1 and UL2 were surgically repositioned with straight forceps. A flexible titanium trauma splint was bonded to all maxillary incisors and deciduous canines for stability and space maintenance for the missing UR2. After repositioning, the affected papillae were approximated and sutured into position to aid healing (Figure 2).
Figure 2. Post-operative photograph, showing the teeth repositioned, soft tissue sutured and the splint in situ.
There is no evidence to support the benefit of systemic antibiotic treatment upon pulpal or periodontal healing.6 However, antibiotics were prescribed as the wound had been grossly contaminated.
Oral hygiene instruction was given to the patient and parents post-operatively, and a follow-up appointment in the paediatric department was arranged for 2 weeks later as per International Association of Dental Traumatology (IADT) guidelines.7
The patient and his father attended for the 2-week review with the paediatric dental team. There were no complaints of pain, swelling or signs of infection, but the father explained they had difficulty cleaning the splint. To aid the cleaning, the patient was given a single tufted toothbrush. Additionally, the father explained that because of his child's autism, they had a very limited diet. Suggestions were given for soft foods that would be suitable.
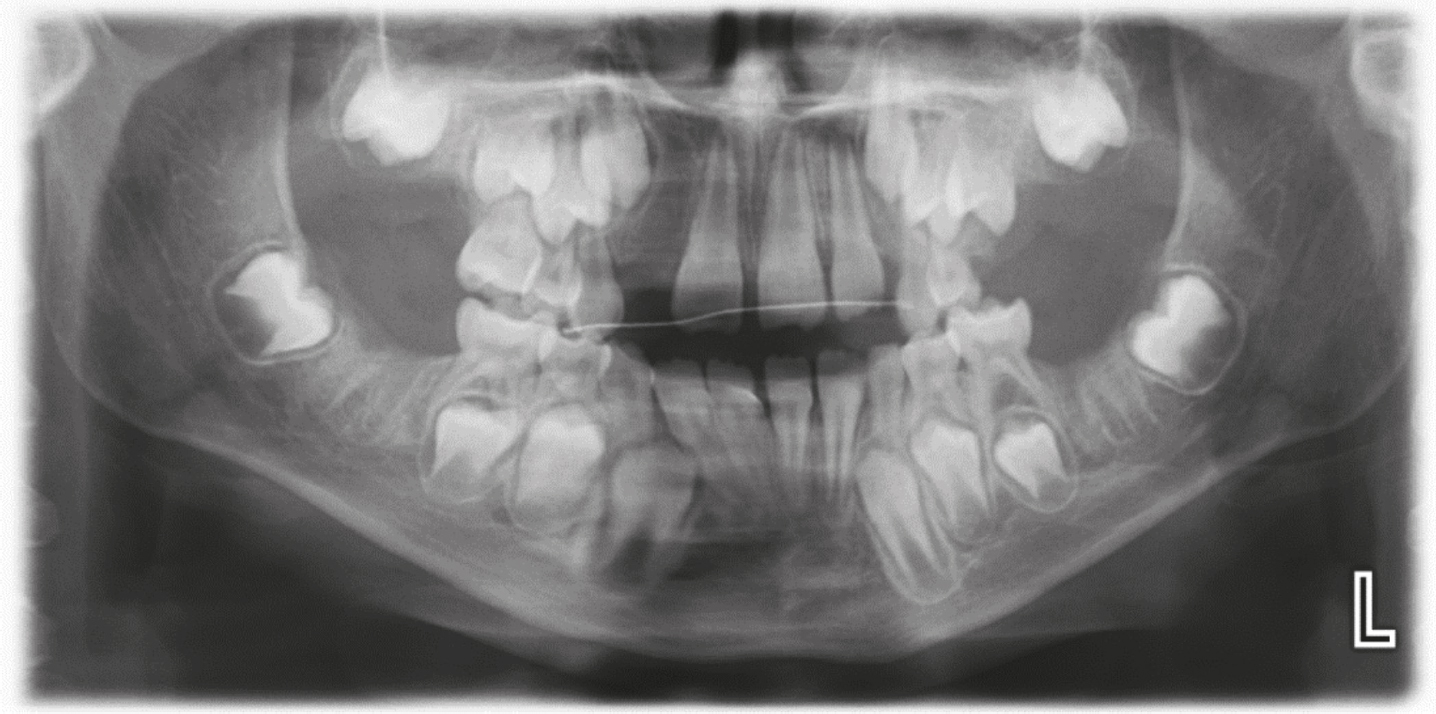
During the initial review, the patient was compliant, and an orthopantomogram (OPG) was taken (Figure 3). The OPG showed the teeth were well positioned, with the splint in situ. The OPG also showed the absence of first permanent molars, which corresponded to a history of previous GA 2 weeks before experiencing the trauma.
Figure 3. Post-operative radiograph taken at 2-week follow-up, showing the teeth repositioned and splint in situ.
Throughout the appointment, compliance became increasingly difficult. Therefore, a full assessment could not be performed. The patient would not allow a trauma stamp of the affected teeth.
A further review was scheduled at 4-weeks post-injury, to assess compliance for splint removal. As it was felt that endodontic treatment would be challenging under local anaesthetic, a referral was made to the paediatric-restorative joint clinic, to ensure all immediate and long-term treatment options are considered.
At the 4-week review, the splint was removed with a combination of acclimatization (tell, show, do) and inhalation sedation (IHS). An in-depth discussion explaining the risks and benefits of undertaking endodontic treatment under GA was undertaken. The need for multiple general anaesthetics was balanced with the long-term prognosis of the teeth. The parents wanted to save the teeth for as long as possible because they felt the psychosocial impact of the patient losing his front teeth was high. A decision was made to proceed with endodontic treatment under general GA.
The patient was scheduled for a highpriority general anaesthetic, but scheduling difficulties caused this to be delayed. Under GA, radiographs were taken, which showed some signs of external inflammatory root resorption (Figure 4). The UR1, UL1 and UL2 were dressed with calcium hydroxide to halt resorption.
The patient and his father attended for review post-GA. They were no complaints of pain or problems with the teeth, but the father explained they still had ongoing difficulty with cleaning them. Detailed oral hygiene instruction was given. Patient compliance had vastly improved by being acclimatized to the dental environment. Post-operative photographs were taken with parental consent, showing the teeth in a favourable position (Figure 5).
Figure 5. Post-operative photograph taken following endodontic therapy under GA.
Further GA would be required to complete the endodontic treatment. Continual monitoring and review was to be undertaken by the paediatric team, in accordance with IADT guidelines.7
Discussion
In this case of dental trauma, the patient required close follow-up for up to 5 years.8 Although the prognosis of all anterior teeth was guarded, the psychosocial impact of losing all anterior teeth guided the treatment plan.
Prognosis for the teeth involved is guarded because teeth should ideally be repositioned as soon as possible after the injury. In this case, there was a delay owing to the need for a GA to perform full assessment and management within the main emergency theatre. Additionally, in optimal circumstances, a treatment plan for the intruded UR1, UL1 and UL2 would require endodontic management within 2 weeks. As a consequence of patient and scheduling factors, this was not possible.
Long-term prognosis was further complicated by the loss of vitality owing to the maturity of the tooth roots. One of the common sequelae in intrusive luxation injuries is pulpal necrosis. In this case, as the pulp was necrotic, the inflammatory response had been initiated and had led to external inflammatory resorption, as seen in Figure 4. Another long-term sequela is replacement resorption and ankylosis, for which the patient will be closely monitored.
As a result of the patient's ASD, behavioural management techniques played a large role in providing care and follow up. A general anaesthetic was indicated in this case to manage the urgent trauma. A combination of acclimatization, IHS and GA has been used for the patient's ongoing treatment.
During the course of care, the patient's compliance was variable. As such, adjustments were made. Reasonable adjustments, such as seeing the same clinician in the same room, were made. Acclimatizing the patient vastly improved the patient's compliance. Poor oral hygiene may worsen the prognosis for the restored teeth, which if left untreated could progress to failing restorations and eventual tooth loss. Efforts were made at each appointment to reinforce oral hygiene techniques with the patient and parents to improve the long-term prognosis of the repaired teeth.
The multidisciplinary approach employed by the maxillofacial and paediatric teams ensured the child had the best emergency management for their dental injury and plan for ongoing care.
Often, these injuries occur outside working hours and during weekends when there is rarely any paediatric dental support. During such times, comprehensive documentation with clinical images would help the paediatric dental team for the child's onward care.